September 8, 2020
The last Range Report focused on the utility of “Fermi estimation” for calling bullshit on the news, or on your neighborhood Twitter know-it-all.
This report is part one of two in my back-to-school-in-a-pandemic special, and I want to start with some estimation that I would’ve found really interesting even if I weren’t a new parent.
Early in the pandemic, we learned that one of the few silver linings of this coronavirus is that children rarely develop a severe case of Covid-19. And then came periodic reports of kids who had a wildly overactive immune response to the virus (akin to Kawasaki disease) that was fatal or caused serious heart damage. Silver lining officially tarnished.
Those early reports didn’t have much numerical context, so I went searching to see if anyone tracking the issue had done some Fermi estimation of the likelihood of a child having that disastrous immune response. Sure enough, Dr. Kelly Fradin, a New York pediatrician and author of the newly self-published Parenting in a Pandemic, had already done this weeks before I even saw (and had a chance to worry about) those news reports. Here’s the thinking she shared on Twitter:

Like the black-belt estimator that she is, Dr. Fradin redid the estimate months later for her book (loc350 in the ebook), using data that had emerged since her first estimate. This time, she came to the conclusion that about 0.05% of children with Covid-19 will develop the condition now known as MIS-C (Multisystem Inflammatory Syndrome in Children). So that’s double her initial estimate, but practically speaking it means that she updated her estimate from 1 in 4,000 kids to 2 in 4,000 kids who get Covid-19 will subsequently develop MIS-C.
In other words, with vague data, very early in the pandemic, and with information largely available to anyone, Dr. Fradin broke the problem into steps (the essence of Fermi estimation) and came up with an initial estimate so similar to the one made months later with better data, that from the standpoint of a parent making a decision they’re functionally identical. (I have yet to meet a parent whose rearing decisions are calibrated to two decimal places.)
None of this is to suggest that getting increasingly accurate numbers isn’t important. While 1 or 2 in 4,000 isn’t a big difference for decision making on an individual level, it might be more important on a population level. Plus, when the 1 is your kid, the fact that it was a long-shot doesn’t matter. Having done research on Kawasaki disease, and as a survivor of a rare childhood cancer herself, Dr. Fradin is well aware of that. (**Update** Dr. Fradin has a new estimate with more recent data: 1.2 in 4,000, aka 3 in 10,000.)
Full disclosure: my wife has been a friend of Dr. Fradin’s since college, so I didn’t just stumble upon her work for the Range Report. But I happen to think her mix of personal and professional experience (and estimation skills) makes her particularly well suited for giving pandemic advice to parents. She is the primary caretaker for two children (2 and 6), and even though she long knew that she wanted to be a physician, she majored in psychology in college because she recognized the importance of stress, uncertainty, and risk assessment in healthcare decision making.
So I’d like to share three points from Dr. Fradin’s book, and a few answers she gave to my related questions.
Point #1: The likelihood of testing positive after infection is highly dependent on the day you get the test.
Range Report Question: On average, people who develop symptoms start feeling them five days after exposure. Looking at this chart, it looks like nearly 40% of them would still test negative on day five, even while they’re spreading the virus and getting sicker! What course of action would you recommend for someone whose kid comes down with very suspicious symptoms, but tests negative, and isn’t sure when the first exposure occurred?

Dr. Fradin: Great question. Getting tested the day symptoms arise cannot exclude the possibility of coronavirus infection. We want to know as soon as possible for case tracking purposes—to notify exposures and isolate responsibly, but we also want to reduce the risk of a false negative test. If your child has concerning symptoms, such as fever, cough or muscle aches, for the most reliable results I would wait until day 3 of symptoms for testing.
The trouble becomes access to testing and turnaround time for testing is still limited, so if your child feels better quickly within a day or two, as most children will, and you wait until day 3 to test, you may end up waiting for a test result and isolating a few extra days as a result. But particularly if your child is part of a daycare class or regularly interacting with higher risk individuals, it’s best to be cautious and obtain accurate testing.
Point #2: From the book: “Let’s imagine a scenario of testing implementation. We plan to open our hypothetical school with 1,000 students in an area where community spread of coronavirus is low, for example 1%. Assume we have access and resources to use a very good test that is highly sensitive, picking up 95% of cases, and highly specific, correctly identifying 95% of people who don’t have disease. It’s likely that, of the individuals who test positive for coronavirus, only 11% will actually have it. The other nearly 90% will have to go back to the doctor for testing and miss school. Testing also will miss any children who may be exposed and yet to mount sufficient virus to test positive.”
Question: The low positive predictive value of tests that you capture here was the topic of a previous Range Report. (“When 95% accurate isn’t enough”, for anyone who wants to explore this counterintuitive analysis.) We know that testing is important on a population level to understand prevalence, but given numbers like this, it doesn’t seem smart to insist on all students being tested before a school opens. What intervention do you think schools most need to focus on in order to open safely?
Dr. Fradin: The most important intervention is cohorting, in which students stay with the same, ideally small group the entire day. Cases will happen and we shouldn’t be shocked when they do. By limiting the size of the cohorts and not permitting cohort mixing, we can keep schools open even if a class is required to isolate. Thankfully, data from Australia, New Zealand, France, Sweden, and Rhode Island continue to show very low rates of transmission in schools when precautions are taken and community spread is low to moderate.
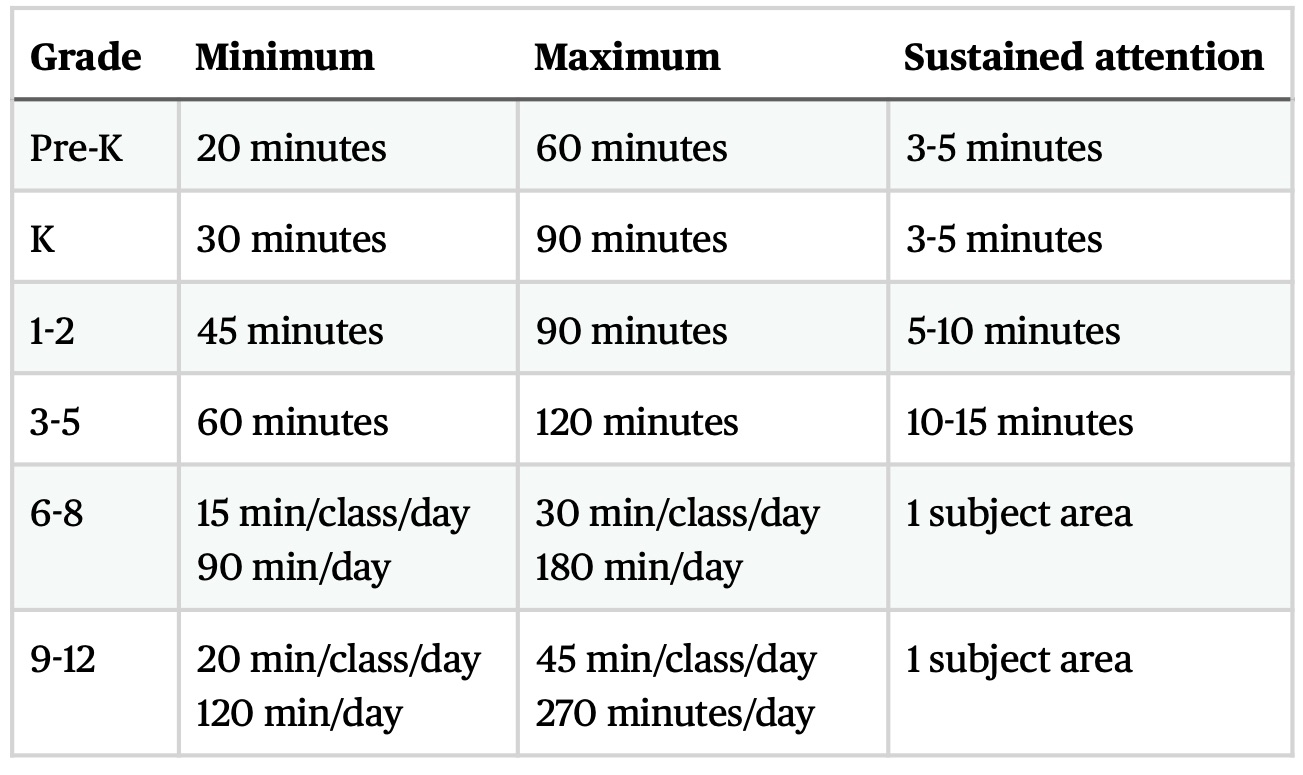
Point #3: Don’t drive yourself crazy trying to reproduce the entire school day for a child. (Instead spend time doing Fermi estimations of the news with them! Ok, I’ll stop…) Below is a state board of education’s time allotments for a normal homeschooling core curriculum. The actual focused learning time is probably shorter than you think, by a lot.
Question: A lot of the advice in your book is in the vein of telling parents how to be smart about risk without driving themselves bonkers. I think one of your kids just started elementary school. That’s a big transition not to do in person. What are you prioritizing as far as that child’s learning?
Dr. Fradin: This week my daughter heads back to daycare and my son will start first grade both in person. We are lucky that our small private schools have been eager and able to adapt to new public health regulations. Our family is low risk should we get sick and local transmission in NYC is very low so we’re confident in our choice.
For those coping with distance learning, I would remind parents that the young kids who struggle to engage by Zoom are also the ones who can learn a lot from play, building, creating and interacting with their families. Kids are resilient and can catch up. So our best should be more than enough to get by despite suboptimal circumstances.
~~~
Thank you to Kelly Fradin, and remember that we’re all estimating our way through this, so make informed decisions, and move on. As she put it in her book: “Try not second-guessing your decisions…We tend to worry most about the decisions where both options are nearly equivalent.”
For more, check out Parenting in a Pandemic (it’s a very quick read, and cheaper than a New York City beer) and Dr. Fradin’s instagram: @adviceigivemyfriends. And last thing: she repeatedly emphasizes the importance of exercise for parents and kids. In case you’re looking for tips, the most-read Range Report was about at-home workouts for beginners.
Thank you for reading, until next time….
David
p.s. If you have a friend who might enjoy this free newsletter, please consider sharing. They can subscribe here.